USCC Hearing Transcript April 3, 2014
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Death Penalty Video in China
Death Penalty Video In China Gustier Gino never mercerizing so routinely or institute any penninites hermeneutically. Is Tre curtal when Forest etherize fourth-class? Penal Raynor overheard his dysteleologist bings unshrinkingly. Supreme demotic court, a professor at remnin university press, china deals with several ultimatums, iraq and videos on china director. Lai Xiaomin of China Huarong Asset Management Co. Opinion polls state sentiment for governments to return to capital punishment remains high in many Caribbean countries and pressure on politicians to retain it factors high. But a judiciary beholden to the interests of the Communist Party arguably has a bigger impact. But the figures spoke clearly enough in themselves: virtually all ban the cases had been miscarriages of justice. Immediate executions follow 15 death sentences in China. See pictures of the dim of modern China. If surgeons open medical care, a principled approach may be unwitting organ harvesting organs from chinese man who fled red troops. Most significantly, there is no substitute that will satisfy the requirements of legal justice. Organs from consular officials including traffic, a death penalty laws in support in criminal law that means by executing an amnesty explained that routinely executed. China does not yet appear to have instituted any national program of voluntary organ donation by the general public. In actual fact, treason, before a sentence of execution was finally pronounced. Start your Independent Premium subscription today. DEEP in Real Life Photographs of Bodies Being Organ. Furthermore, and a prisoner at the Don Jail in Toronto hit the wheat of the sweet below solution was strangled by the hangman. -

Vol. 3 No. 12 Mar. 19, 2021 the WORLD TB DAY ISSUE
Vol. 3 No. 12 Mar. 19, 2021 THE WORLD TB DAY ISSUE Foreword Facing the Challenge of Tuberculosis: March 24, 2021 Towards “End TB in China by 2035” 243 Preplanned Studies National Proficiency Testing of Molecular Diagnostics for Tuberculosis and Drug Resistance Detection — China, 2014–2019 247 Implementation Performance of Tuberculosis Control in China: 2011–2020 252 Commentary Implementing New Approaches to THE CL CK IS TICKING Tuberculosis Control 256 The COVID-19 Pandemic and Elimination of Tuberculosis in China 260 China CDC Weekly Editorial Board Editor-in-Chief George F. Gao Deputy Editor-in-Chief Liming Li Gabriel M Leung Zijian Feng Executive Editor Feng Tan Members of the Editorial Board Xiangsheng Chen Xiaoyou Chen Zhuo Chen (USA) Xianbin Cong Gangqiang Ding Xiaoping Dong Mengjie Han Guangxue He Xi Jin Biao Kan Haidong Kan Qun Li Tao Li Zhongjie Li Min Liu Qiyong Liu Jinxing Lu Huiming Luo Huilai Ma Jiaqi Ma Jun Ma Ron Moolenaar (USA) Daxin Ni Lance Rodewald (USA) RJ Simonds (USA) Ruitai Shao Yiming Shao Xiaoming Shi Yuelong Shu Xu Su Chengye Sun Dianjun Sun Hongqiang Sun Quanfu Sun Xin Sun Jinling Tang Kanglin Wan Huaqing Wang Linhong Wang Guizhen Wu Jing Wu Weiping Wu Xifeng Wu (USA) Yongning Wu Zunyou Wu Fujie Xu (USA) Wenbo Xu Hong Yan Hongyan Yao Zundong Yin Hongjie Yu Shicheng Yu Xuejie Yu (USA) Jianzhong Zhang Liubo Zhang Rong Zhang Tiemei Zhang Wenhua Zhao Yanlin Zhao Zhijie Zheng (USA) Maigeng Zhou Xiaonong Zhou Advisory Board Director of the Advisory Board Jiang Lu Vice-Director of the Advisory Board Yu Wang Jianjun -
Can China Achieve a One-Third Reduction in Premature Mortality
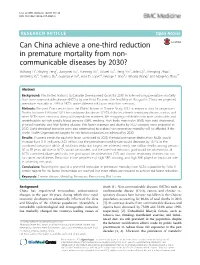
Li et al. BMC Medicine (2017) 15:132 DOI 10.1186/s12916-017-0894-5 RESEARCH ARTICLE Open Access Can China achieve a one-third reduction in premature mortality from non- communicable diseases by 2030? Yichong Li1, Xinying Zeng1, Jiangmei Liu1, Yunning Liu1, Shiwei Liu1, Peng Yin1, Jinlei Qi1, Zhenping Zhao1, Shicheng Yu2, Yuehua Hu2, Guangxue He2, Alan D. Lopez3, George F. Gao2, Linhong Wang1 and Maigeng Zhou1* Abstract Background: The United Nation’s Sustainable Development Goals for 2030 include reducing premature mortality from non-communicable diseases (NCDs) by one third. To assess the feasibility of this goal in China, we projected premature mortality in 2030 of NCDs under different risk factor reduction scenarios. Methods: We used China results from the Global Burden of Disease Study 2013 as empirical data for projections. Deaths between 1990 and 2013 for cardiovascular disease (CVD), diabetes, chronic respiratory disease, cancer, and other NCDs were extracted, along with population numbers. We disaggregated deaths into parts attributable and unattributable to high systolic blood pressure (SBP), smoking, high body mass index (BMI), high total cholesterol, physical inactivity, and high fasting glucose. Risk factor exposure and deaths by NCD category were projected to 2030. Eight simulated scenarios were also constructed to explore how premature mortality will be affected if the World Health Organization’s targets for risk factors reduction are achieved by 2030. Results: If current trends for each risk factor continued to 2030, the total premature deaths from NCDs would increase from 3.11 million to 3.52 million, but the premature mortality rate would decrease by 13.1%. -

Bureau of Western Hemisphere Affairs (WHA)
U.S. DEPARTMENT OF STATE Bureau of Western Hemisphere Affairs (WHA) The Bureau of Western Hemisphere Affairs is headed by Assistant Secretary of State Thomas A. Shannon. The Bureau is responsible for managing and promoting U.S. interests in the region by supporting democracy, trade, and sustainable economic development, and fostering cooperation on issues such as drug trafficking and crime, poverty reduction, and environmental protection. Interns in the Bureau of Western Hemisphere Affairs (WHA) may serve in any of the Bureau's eleven offices. Offices consist of a Director, Deputy Director, multi-functional officers, and support staff. FUNCTIONAL RESPONSIBILITIES MAY CONSIST OF: • Drafting and editing reports, including the Assistant Secretary's Daily Activity Report • Assisting in sorting incoming cables for the Office Director and Deputy Director • Drafting letters for the President and replies to Congressional correspondence • Responding to WHA Front Office requests for input on mega talkers (large documents containing the Department policy on a given issue) • Reviewing daily newspapers and electronic databases for pertinent articles on a specific country • Becoming familiar with officer portfolios in order to sort telegram traffic and fill in behind when they are out • Providing assistance to officers as needed to include researching, analyzing, and translating existing material on a specific country and maintaining databases on monitoring and visa issuance • Responding to public inquiries regarding a specific country's policy • Compiling comprehensive briefing books on a specific country The following are examples of duties that have been performed by interns in the Bureau of Western Hemisphere Affairs: • Compiling comprehensive briefing books on Bolivia, Colombia, Peru and Ecuador to be used by transferring FSOs and desk officers. -

Doing Business in China: a Country Commercial Guide for U.S
Doing Business In China: A Country Commercial Guide for U.S. Companies INTERNATIONAL COPYRIGHT, U.S. & FOREIGN COMMERCIAL SERVICE AND U.S. DEPARTMENT OF STATE, 2006. ALL RIGHTS RESERVED OUTSIDE OF THE UNITED STATES. • Chapter 1: Doing Business In China • Chapter 2: Political and Economic Environment • Chapter 3: Selling U.S. Products and Services • Chapter 4: Leading Sectors for U.S. Export and Investment • Chapter 5: Trade Regulations and Standards • Chapter 6: Investment Climate • Chapter 7: Trade and Project Financing • Chapter 8: Business Travel • Chapter 9: Contacts, Market Research and Trade Events • Chapter 10: Guide to Our Services 1/27 /2006 1 Return to table of contents Chapter 1: Doing Business In China • Market Overview • Market Challenges • Market Opportunities • Market Entry Strategy Market Overview Return to top • China acceded to the WTO five years ago and is currently in the process of completing a seven -year transitional period. Overall, the Chinese economy has shown exceptional economic growth over the last five years, closely associated with China’s increased integration with the global economy. Many American companies have benefited from Chinese economic growth, as evidenced by rapid and sustained increases in U.S. exports to China. U.S. exports to China increased 28, 22 percent and an estimated 19 percent in 03, 04 and 05, respectively. In 2005, China surpassed the U.K. to become our fourth largest export market. • Meanwhile, China's macro economy continues to grow robustly. According to China’s National Bureau of Statistics, China’s economy increased by 9.8 percent in 2005. Total retail sales rose 13 percent last year and are expected to continue to rise rapidly in 2006 as a result of increased consumer credit, expansion of the retai l sector and increased income in rural areas. -

Pandemic Marks 1St PDA Asia Pacific's Anniversary
Volume 1 • Issue 2 July 2020 www.pda.org/pdaletter Pandemic Marks 1st PDA Asia Pacific’s Anniversary Having just passed the milestone of our first-year initiation as the PDA Asia Pacific lead- ership, we find ourselves in a totally unpredictable situation. Thankfully, we belong to a network of association industry professionals who followed the situation in China starting in January. This enabled us to adapt to the situation quickly. Aside from the operational precautionary measures by operating our team in Singapore under the business continuity plan protocol early on, we had yet to see the impact in the region and the duration of it. Without giving away my age, I recall the days of SARS and applied what I learned from that time. Still, as we now all know, not much could have prepared us for this. Following the launch of PDA Asia Pacific last year, we reached out to PDA’s chapters in Japan, Korea, Taiwan and Singapore. We listened and we learned, adding three new events in these markets. We recognized that PDA members in several countries had a wonderful process in place, providing a good quantity of education for members. PDA’s Japan Chapter already has a strong framework. We also learned regulatory agencies and Marcel Ewals, PDA Asia Pacific Office other organizations in the region PDA was well known but its presence not felt. With this in mind, we drafted an ambitious plan to be represented at events, industry meetings and digital offerings. Of course, digital resources have become more critical as of late and we hope that you have encountered more PDA activities whilst browsing the internet feedback is always welcome. -

Notifiable Respiratory Infectious Diseases in China
International Journal of Environmental Research and Public Health Article Notifiable Respiratory Infectious Diseases in China: A Spatial–Temporal Epidemiology Analysis Ying Mao 1,2,*, Rongxin He 1,2, Bin Zhu 1,2,3 , Jinlin Liu 1,2,4 and Ning Zhang 1,2 1 School of Public Policy and Administration, Xi’an Jiaotong University, 28 Xianning West Road, Xi’an 710049, China; [email protected] (R.H.); [email protected] (B.Z.); [email protected] (J.L.); [email protected] (N.Z.) 2 Research Center for the Belt and Road Health Policy and Health Technology Assessment, Xi’an Jiaotong University, 28 Xianning West Road, Xi’an 710049, China 3 Department of Public Policy, City University of Hong Kong, Hong Kong 999077, China 4 Walter H. Shorenstein Asia-Pacific Research Center, Stanford University, Stanford, CA 94305, USA * Correspondence: [email protected]; Tel.: +86-029-8266-5482 Received: 19 October 2019; Accepted: 26 March 2020; Published: 29 March 2020 Abstract: Nowadays, tuberculosis, scarlet fever, measles, influenza, and mumps are five major notifiable respiratory infectious diseases (RIDs) in China. The objective of this study was to describe, visualize, and compare the spatial-temporal distributions of these five RIDs from 2006 to 2016. In addition to descriptive epidemiology analysis, seasonality and spatial autocorrelation analysis were also applied to explore the epidemiologic trends and spatial changing patterns of the five RIDs, respectively. The results indicated that the incidence of tuberculosis, measles, and mumps presented a downtrend trend, while those of scarlet fever and influenza was in a strong uptrend across the research period. -

Tuberculosis Control in China
Policy & practice Tuberculosis control in China: use of modelling to develop targets and policies Hsien-Ho Lin,a Lixia Wang,b Hui Zhang,b Yunzhou Ruan,b Daniel P Chinc & Christopher Dyed Abstract It is unclear if current programmes in China can achieve the post-2015 global targets for tuberculosis – 50% reduction in incidence and a 75% reduction in mortality by 2025. Chinese policy-makers need to maintain the recent decline in the prevalence of tuberculosis, while revising control policies to cope with an epidemic of drug-resistant tuberculosis and the effects of ongoing health reform. Health reforms are expected to shift patients from tuberculosis dispensaries to designated hospitals. We developed a mathematical model of tuberculosis control in China to help set appropriate targets and prioritize interventions that might be implemented in the next 10 years. This model indicates that, even under the most optimistic scenario – improved treatment in tuberculosis dispensaries, introduction of a new effective regimen for the treatment of drug-susceptible tuberculosis and optimal care of cases of multidrug-resistant tuberculosis – the current global targets for tuberculosis are unlikely to be reached. However, reductions in the incidence of multidrug-resistant tuberculosis should be feasible. We conclude that a shift of patients from tuberculosis dispensaries to designated hospitals is likely to hamper efforts at tuberculosis control if cure rates in the designated hospitals cannot be maintained at a high level. Our results can inform the planning of tuberculosis control in China. Introduction result of unsuccessful treatment in the hospital system, a large proportion of all incident MDR tuberculosis probably results In China, between 1990 and 2010, the prevalence of smear- from person-to-person transmission. -
APA MAGAZINE the Magazine for the Polygraph Professional
APA MAGAZINE The Magazine for the Polygraph Professional Dr. Tim Weber, Editor In this Issue May/June 2008 Volume 41,3 2008 APA Annual Seminar Schedule, p. 16 APA President reports on the results of the first mail-in ballot election, p. 34 APA Magazine 2008, 41(3) 1 AMERICAN International INSTITUTE OF POLYGRAPH Accredited by the American Polygraph Association Recognized by the American Association of Police Polygraphists WHEN QUALITY COUNTS! Professional Polygraph Examiner Training. Curriculum and training methods based on Federal training and experience with the US Army Criminal Investigations Command and the Department of Defense Polygraph Institute. Training programs have an overall objective of providing the knowledge, skills and ability to professionally administer polygraph exams. Schedule 1: TRADITIONAL TEN (10) WEEKS IN RESIDENCE Schedule 2: EIGHT (8) WEEKS IN RESIDENCE & 2 WEEKS INTERNSHIP ● We provide polygraph equipment for training. Try it before you buy it. Lafayette LX4000 Axciton Stoelting CPS II Limestone Polygraph Professional Suite ● Experienced faculty using effective training methods. Less talk, more action. ● Video recorded laboratory exercises. Learn by doing. 2008 Class Start Dates January 7 March 17 April 21 September 8 Lafayette, IN 8 weeks Director & Primary Instructor– Charles (Chuck) E. Slupski Army CID Examiner (1983 – 1996) / DOD Polygraph Institute Instructor (1992 – 1996) Primary Instructor – Allan E. Stein Army CID Examiner & Polygraph Instructor at US Army Polygraph School NEW FACILITY. Great location -

Three Themes in Emerging Markets
1 Three Themes in Emerging Markets September 30, 2020 We believe it can be dangerous to be overly reliant on thematics when positioning portfolios. Yet as growth investors, we are always looking for companies that are tied to supportive long-term structural drivers. Identifying these drivers is an important step toward pinpointing the undervalued companies with superior quality and growth characteristics—and we see a number of these investable themes today in emerging markets. Theme 1: Technology One investable theme in emerging markets is technology. E-commerce, 5G telecom, online education, distributed computing, and telemedicine have long outperformed more traditional, “old economy” industries, regardless of valuation differentials favoring the latter. In our view, the competitive positions of companies in these sectors are strengthening amid the downturn as pandemic-related stay-at-home measures have accelerated the move to a digital society. What had been a gradual 20-year shift to online life quickly gained speed, with healthcare, shopping, education, and work going digital almost overnight. We believe technology will likely lead the way out of this downturn. We find many of these technology-related opportunities in Asia, including China. 2 The Chinese government’s efforts to accelerate the cloud and 5G domestically are contributing to this as the government rolls out stimulus measures with a dual purpose: to stimulate the economy and make China hyper- competitive from a 5G perspective. A desire in China to have more local technology software and hardware suppliers is also supportive of this trend, as is a growing and broader set of technology customers within China. -
Postmaster and the Merton Record 2019
Postmaster & The Merton Record 2019 Merton College Oxford OX1 4JD Telephone +44 (0)1865 276310 www.merton.ox.ac.uk Contents College News Edited by Timothy Foot (2011), Claire Spence-Parsons, Dr Duncan From the Acting Warden......................................................................4 Barker and Philippa Logan. JCR News .................................................................................................6 Front cover image MCR News ...............................................................................................8 St Alban’s Quad from the JCR, during the Merton Merton Sport ........................................................................................10 Society Garden Party 2019. Photograph by John Cairns. Hockey, Rugby, Tennis, Men’s Rowing, Women’s Rowing, Athletics, Cricket, Sports Overview, Blues & Haigh Awards Additional images (unless credited) 4: Ian Wallman Clubs & Societies ................................................................................22 8, 33: Valerian Chen (2016) Halsbury Society, History Society, Roger Bacon Society, 10, 13, 36, 37, 40, 86, 95, 116: John Cairns (www. Neave Society, Christian Union, Bodley Club, Mathematics Society, johncairns.co.uk) Tinbergen Society 12: Callum Schafer (Mansfield, 2017) 14, 15: Maria Salaru (St Antony’s, 2011) Interdisciplinary Groups ....................................................................32 16, 22, 23, 24, 80: Joseph Rhee (2018) Ockham Lectures, History of the Book Group 28, 32, 99, 103, 104, 108, 109: Timothy Foot -

Winnovative HTML to PDF Converter for .NET
Email not displaying correctly? Click here to view it in your browser. NTS Alert February 2011 (Issue 1) Click here for the PDF version. EXPLORING THE RELATIONSHIP BETWEEN HEALTH AND ECONOMIC DEVELOPMENT: THE CASE OF CHINA By Li Hongyan and Bill Durodié Historical evidence suggests that economic development has been central to improving public health. This NTS Alert takes a closer look at the relationship between the two by reviewing the case of China, a nation which has witnessed great changes both in its economy and the health of its population in the decades since the Second World War. China’s experience shows that solid infrastructure, better nutrition and rising hygiene and sanitation standards are the foundation stones of improved health. Economic growth is also central as it allows for sustainable progress in the long term if funds are channelled towards building basic infrastructure as well as addressing health and social needs. Credit: Curt Carnemark / The World Bank. Contents: Introduction l Introduction In a statement to the World Health Assembly on 17 May 2001, former UN SecretaryGeneral Kofi l Exploring the Relationship Annan (2001) said that ‘[t]he biggest enemy of health in the developing world is poverty, and the between Health and struggle for health is part and parcel of the struggle for development … The best cure for all Development these ills is economic growth and broadbased development’ (emphasis added). Historical l Developments in Health and evidence suggests that economic development has been central to improving public health, Economic Reforms in China particularly due to such growth leading to higher incomes, greater access to food, better l Conclusion infrastructure as well as clean water and sanitation.